
The Importance of Bystander CPR
The human body is a truly amazing thing, but behind all of its complexity, there are three core processes that are responsible for keeping us alive from one moment to the next: respiratory drive, oxygenation and perfusion; with each of these processes corresponding to one of our critical body systems: the nervous system, respiratory system and circulatory system. What this boils down to is that all of the cells in our body, both our core organs and those in the periphery such as the skin, require oxygen to stay alive. Anything which interferes with any one of these three core processes is an immediate threat to life or limb.
Let’s break this down and look at it step by step.
Our brain sends signals that cause the diaphragm to contract, expanding the space in the thoracic cavity, thereby reducing the intrathoracic pressure below that of the atmosphere. Following the laws of physics, the atmospheric gases (air) move from the higher pressure environment (the atmosphere), to the lower pressure environment (the lungs) – in this case causing inhalation. These signals that cause the contraction of the diaphragm are our respiratory drive.
The air that we inhale travels through our upper respiratory tract, into the trachea, the various levels of bronchi and bronchioles, then finally into the millions of alveoli in each of our lungs. These alveoli are enveloped by tiny blood vessels (capillaries) and the oxygen diffuses across the wall of those capillaries and attaches to the haemoglobin in the red blood cells travelling through them, oxygenating the blood. This is the process of oxygenation.
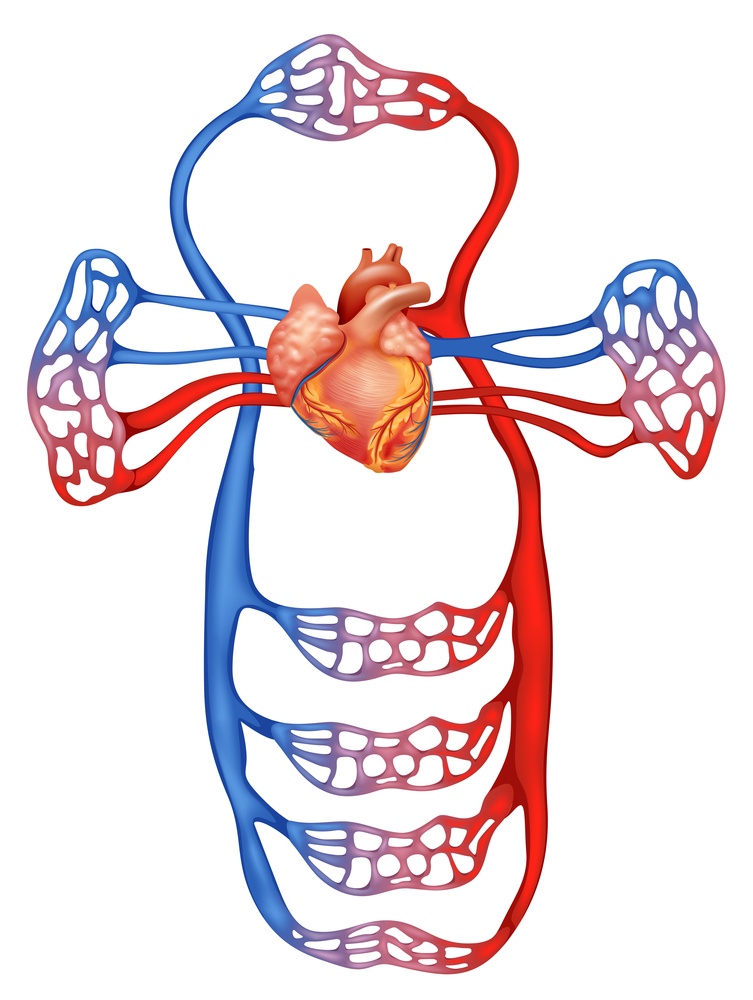
This oxygenated blood is then returned into the left atrium of the heart via the pulmonary veins, which incidentally are the only veins in the human body that carry oxygenated blood. The heart is a mostly hollow organ composed of cardiac muscle and connective tissue. When the heart contracts, it ejects this oxygenated blood under pressure, from the left ventricle, through the aorta and into the coronary circulation (supplying oxygenated blood to the heart muscle itself), and into the systemic circulation, where it travels around the body, allowing the various structures by which it passes to extract oxygen. This is the process of perfusion, which cannot take place without the pressure generated by the heart contracting.
It’s a common misconception that a heart attack and cardiac arrest are the same thing. In fact they are as different as plumbing and electricity.
Heart Attack
The medical term for a heart attack is a myocardial infarction (MI). Whilst that may seem a mouthful, it’s actually pretty straightforward. The prefix MYO refers simply to muscle, the root word CARD or CARDI refers to the heart, and the suffix AL simply means relating to. So myocardial means relating to the heart muscle.
Infarction comes from the latin infarctus, which means to plug up or cram. The medical definition of infarction is tissue death due to the failure of the supply of oxygenated blood, usually due to an obstruction, i.e. a clot; or in other words the vessel carrying the oxygenated blood being plugged up.
So, a heart attack occurs when one of the coronary arteries supplying oxygenated blood to the heart gets blocked and a portion of the muscle being supplied by that artery dies. The longer the blockage remains in place, the more severe and widespread the damage becomes.
This is a plumbing problem.
A person suffering from a heart attack will generally present with crushing, central chest pain that radiates towards the neck, jaw, left arm or back; shortness of breath; nausea; feeling faint or weak; pale, cool, clammy skin; profuse sweating; and may feel a sense of impending doom. However, there are some special populations such as those with diabetes mellitus, who may not present with any symptoms at all due to nerve damage (peripheral neuropathy). These patients are said to suffer a silent myocardial infarction.
Heart attacks rarely cause death unless the patient goes through sudden cardiac death (SCD) after a heart attack. According to the Department of Statistics Malaysia, ischaemic heart disease accounts for about 19.2% of deaths among Malaysians.[1]

Cardiac Arrest
Whilst a heart attack is a plumbing problem, cardiac arrest is an electrical problem. Cardiac arrest is an abrupt disruption in heart function, meaning that either the heart is no longer generating the electrical impulses that cause it contract (asystole), or that the impulses are somehow faulty, resulting in a drastic and catastrophic reduction in the volume of blood being ejected from the heart (ventricular fibrillation, pulseless ventricular tachycardia or pulseless electrical activity).
A person in cardiac arrest will be unresponsive, not breathing and have no pulse. This means that their respiratory drive is not present, there is no oxygen diffusing into the bloodstream and oxygenated blood is not being circulated around the body. This person is clinically dead, and will become irreversibly so if we do not intervene.
Statistically, the survival rate of Out of Hospital Cardiac Arrest (OHCA) is a complex matter and varies based on a number of factors, including but not limited to geography, whether the cardiac arrest was witnessed, and whether the bystander CPR was performed. A global study of the survival rate among adult OHCA patients revealed a survival rate of 8.8% to the point of hospital discharge. This increased to 10.5% for those whose cardiac arrest was witnessed by EMS personnel or a bystander, and 11.3% for those who received bystander CPR.[2]
Treating Cardiac Arrest
In order to treat cardiac arrest, we need to replace the absent functions until such time as they recover (return of spontaneous circulation), or an authorised medical professional pronounces the patient dead. To do this, we use Cardiopulmonary Resuscitation (CPR). CPR doesn’t guarantee that we can resuscitate every patient, however without CPR, the survival rate of OHCA reduces by 10% every minute.[3]
Irreversible brain damage may occur within four minutes of the brain receiving no oxygen, and infarction may occur within 4-6 minutes; so time is most certainly of the essence. This also explains the increase in survival rates for witnessed cardiac arrest, with the provision of prompt, bystander CPR.
Effective CPR is not difficult to learn, yet various articles cite the instance of bystander CPR between 20% and 46%. Statistics show that four out of every five cardiac arrests occur at home[4], meaning that it could be on you to save the life of your parent, partner, child or other close relative. Would you know how?

Conclusion
Currently, knowledge of CPR amongst Malaysians is nascent. According to Karuthan et al, 73% of surveyed participants had attended CPR training of some kind, however, the study also proved that the knowledge of CPR even in those who had been trained was low. The study also concluded that many Malaysians are willing to perform emergency CPR on a stranger, however the exact percentage varied heavily depending on the situation.[6]
Increasing awareness of the importance of bystander CPR and the knowledge of how to perform CPR should be viewed with high importance. The performance of bystander CPR is a significant contributing factor to the survival of cardiac arrest.
Even if it were a stranger that collapsed in front of you, they are someone else’s parent, partner or child. I hope that you would stop and help to the best of your ability, in the hope that a stranger would do the same for your loved one if they were in need.
References
- Statistics on Causes of Death, Malaysia 2019. Department of Statistics Malaysia 2019. https://www.dosm.gov.my/v1/index.php?r=column/pdfPrev&id=RUxlSDNkcnRVazJnakNCNVN2VGgrdz09
- Yan, S., Gan, Y., Jiang, N. et al. The global survival rate among adult out-of-hospital cardiac arrest patients who received cardiopulmonary resuscitation: a systematic review and meta-analysis. Crit Care 24, 61 (2020). https://doi.org/10.1186/s13054-020-2773-2
- Bottiger BW et al (2020). Up to 206 Million People Reached and Over 5.4 Million Trained in Cardiopulmonary Resuscitation Worldwide: The 2019 International Liaison Committee on Resuscitation World Restart a Heart Initiative. Journal of American Heart Association Vol. 9, No. 15. PMID: 32750297.
- GJ, Frederiksen S, Pascual RG. Cardiac arrest in private locations: different strategies are needed to improve outcome. Resuscitation. 2003 Aug;58(2):171-6. doi: 10.1016/s0300-9572(03)00118-7. PMID: 12909379.
- Weisfeldt ML, et al. Ventricular Tachyarrhythmias after Cardiac Arrest in Public versus at Home. New England Journal of Medicine, 2011; 364:313-321.
- Karuthan SP et al (2019). Knowledge of and willingness to perform Hands-Only cardiopulmonary resuscitation among college students in Malaysia. Medicine (Baltimore) 98(51): e18466. PMID: 31861024.
Written by Damien Santer and Clement Chong.
Fact checked by Dr Peter Natarajan